Conditions & Treatments

Urinary Incontinence and its causes
Stress incontinence
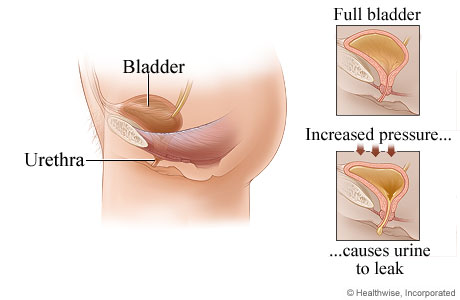
Stress incontinence happens when the pressure inside your bladder as it fills with urine becomes greater than the strength of your urethra to stay closed (the urethra is the tube through which urine passes out of your body).
Your urethra may not be able to stay closed if:
- Your pelvic floor muscles are weak or damaged
- Your urethral sphincter (the ring of muscle that keeps the urethra closed) is damaged
Any sudden extra pressure on your bladder, such as laughing or sneezing, can cause urine to leak out of your urethra. The loss of strength in your urethra may be caused by:
- Nerve damage during childbirth
- Increased pressure on your tummy, for example because you are pregnant or very overweight
- A lack of the hormone oestrogen in women (less oestrogen is produced after the menopause)
- Certain medications
Urge incontinence
 The urgent and frequent need to pass urine can be caused by a problem with the detrusor muscles in the walls of the bladder. The detrusor muscles relax to allow the bladder to fill with urine, and then contract when you go to the toilet to let the urine out.
The urgent and frequent need to pass urine can be caused by a problem with the detrusor muscles in the walls of the bladder. The detrusor muscles relax to allow the bladder to fill with urine, and then contract when you go to the toilet to let the urine out.
Sometimes the detrusor muscles contract too often, creating an urgent need to go to the toilet. This is called detrusor overactivity. The reason your detrusor muscles contract too often may not be clear, but possible causes include:
- Neurological conditions, which affect the brain and spinal cord such as Parkinson's disease or multiple sclerosis
- Conditions affecting the lower urinary tract (urethra and bladder), such as urinary tract infections (UTIs) or tumours in the bladder
- Drinking too much alcohol or caffeine
- Constipation
- Certain medications
Some of these possible causes will lead to short-term urinary incontinence; others may cause a long-term problem.
Risk factors are not the same as causes. Risk factors are things that increase your chance of developing a condition.
Risk factors
Risk factors for urinary incontinence in women include:
- Pregnancy – if you developed stress incontinence during pregnancy, or in the six weeks after birth, you are more likely to have stress incontinence five years after the birth
- Vaginal birth – giving birth vaginally, rather than with a caesarean, may be associated with stress incontinence
- Obesity – having a body mass index (BMI) of 30 or more may also be associated with urinary incontinence family history – there may be a genetic link to urinary incontinence, particularly stress incontinence
- Disability – conditions affecting your brain or spinal cord, such as multiple sclerosis or dementia may increase your risk of urinary incontinence
- Increasing age – urinary incontinence becomes more common as you reach middle age and is most common in women over 70
- Lower urinary tract symptoms (LUTS) – symptoms that affect the bladder and urethra
Surgery for stress incontinence is usually considered when conservative measures have failed E.g. Pelvic floor (Kegel) exercises.
If you plan to have more children, this will affect your decision about whether or not to have surgery. The physical strain of pregnancy and childbirth can sometimes cause surgical treatments to fail and therefore, you may wish to wait until you no longer want to have any more children.
Surgery for stress incontinence
Tape procedures for women
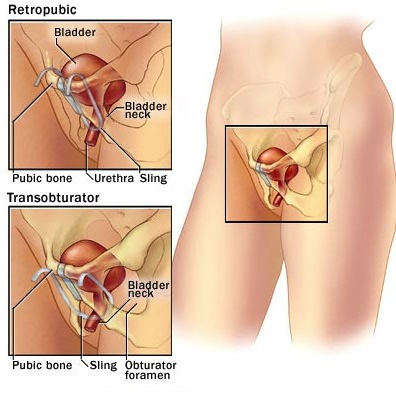 Tape procedures can be used for women with stress incontinence. A piece of tape is inserted through an incision inside the vagina and threaded behind the urethra. The middle part of the tape supports the urethra, and the two ends are threaded through two incisions in either the:
Tape procedures can be used for women with stress incontinence. A piece of tape is inserted through an incision inside the vagina and threaded behind the urethra. The middle part of the tape supports the urethra, and the two ends are threaded through two incisions in either the:
- Abdomen – this is called a retropubic tape procedure or Tension-free vaginal tape procedure (TVT)
- Tops of the inner thigh – this is called a Transobturator tape procedure (TOT)
Some studies have suggested that TVT may be more effective than TOT in some cases. There is a slightly higher risk of injury to the bladder during TVT, and a higher risk of injury to the urethra during TOT. TOT may also cause thigh pain.
With a conventional TVT tape, one expects around 85% of women to be cured.
Downloads
- Operations for Stress Incontinence Mid-Urethral Tapes
- An Operation for Stress Incontinence Transobturator Tape
- An Operation for Stress Incontinence Tension Free Vaginal Tape
Sling procedures
Sling procedures involve making an incision in your lower abdomen and inserting a sling around the neck of the bladder to support it. The sling could be made of:
- A synthetic material
- Tissue taken from another part of your body (an autologous fascial sling)
- Tissue donated from another person (an allograft sling)
- Tissue taken from an animal (a xenograft sling), such as cow or pig tissue
Autologous fascial slings are a long-term treatment for stress incontinence and may be the most effective.
Synthetic slings may carry long-term risks of causing difficulty urinating or urge incontinence.
Sling surgery is not commonly performed now, as it is quite a major operation.
Colposuspension
A colposuspension involves making an incision in your lower abdomen and lifting up the neck of your bladder. Stitches through the walls of the bladder neck hold it in place. Like the sling procedure it is also a major open operation. Colposuspension used to be the commonest procedure to treat stress incontinence but has largely been superceded by the less invasive TVT procedure.
Urethral bulking agents
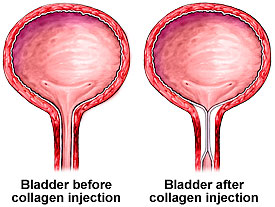 A urethral bulking agent is a substance that is injected into the walls of your urethra (the tube that carries urine from the bladder to outside the body). This increases the size of the urethral walls and allows the urethra to stay closed with more force. A number of different bulking agents are available and there is no evidence that one is more beneficial than another. Bulking agent success rates are approximately 30-40%. I normally to use a product called Bulkamid.
A urethral bulking agent is a substance that is injected into the walls of your urethra (the tube that carries urine from the bladder to outside the body). This increases the size of the urethral walls and allows the urethra to stay closed with more force. A number of different bulking agents are available and there is no evidence that one is more beneficial than another. Bulking agent success rates are approximately 30-40%. I normally to use a product called Bulkamid.
Bulking agents are less invasive than other surgical treatments as they do not require any incisions. However, they are less effective than the other options. The effectiveness of the bulking agents will reduce with time and you may need repeated injections.
Procedures for urge incontinence or overactive bladder syndrome
Botulinum toxin A injections
Botulinum toxin A (Botox) can be injected into the sides of your bladder to treat urge incontinence and overactive bladder syndrome (OAB).
Although the symptoms of incontinence may improve after the injections, you may not be able to pass urine normally, so you will be taught how to insert a catheter (a thin, flexible tube) to drain the urine from your bladder. This is called clean intermittent self-catheterisation (CISC) and will need to be carried out by approximately 20% of patients.
Botulinum toxin A is not currently licensed to treat urge incontinence or OAB, so you should be made aware of any risks before deciding to have the treatment. The long-term effects of this treatment are not yet known, but it may be of benefit when other treatments have not worked.
Evidence suggests that botulinum toxin A may cure incontinence or improve symptoms by 90%. The effects can last for up to 12 months.